
~ Guidelines ~
- Adult Advanced Life Support
- Pediatric Advanced Life Support (PALS) Updates
- Sience Overview Basic Life Support
- Training Implementation
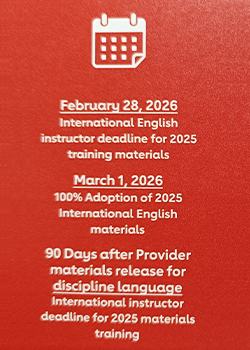
- 2026 AHA Guidelines Launch
- 2025 Heartcode Basic Life Support (BLS)
 |
Adult Advanced Life Support |
|---|
 |
■ALS Hot Topics/Controversies |
|---|
  |
■ALS Top 10 A rapid assessment of clinical stability is essential to direct the appropriate advanced life support (ALS) treatment, and these guidelines go into greater depth to describe how poor organ perfusion manifests as instability.
Higher first-shock energy settings (≥200J) are preferable to lower settings for cardioversion of atrial fibrillation and atrial flutter.
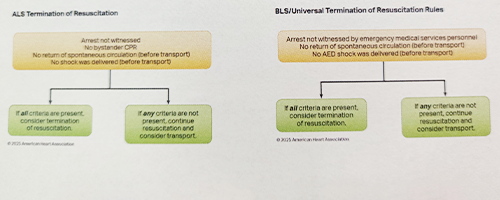
Updated termination of resuscitation (TOR) guidelines emphasize rule application based on emergency medical services (EMS) scope of practice (basic life support [BLS], ALS, or universal TOR rule [UTOR]), and that end-tidal carbon dioxide (ETCO2) should not be used in isolation to end resuscitative efforts.
Vector change (VC) and double sequential defibrillation (DSD) may be considered as therapies for shock-refractory ventricular fibrillation (VF); however, further investigation of the technique, patient candidacy and the development of new technology to optimize shock delivery are necessary.
Head-up cardiopulmonary resuscitation (CPR) use is discouraged outside of the setting of rigorous clinical trials with appropriate subject protections.
Recommendations regarding outdated or extraordinary procedures that have been replaced by modern equivalents with better efficacy (eg, administration of intra-arrest medications via an in-place endotracheal tube) have been removed.
Use of point-of-care ultrasonography (POCUS) by experienced professionals during cardiac arrest may be considered to diagnose reversible causes if it can be done without interrupting resuscitative efforts (ie, CPR).
Pulseless ventricular tachycardia (pVT) is always unstable and should be treated immediately with defibrillation, because delays in shock delivery worsen outcomes.
Intravenous (IV) access remains the first-line choice for drug administration during cardiac arrest; however, intraosseous (IO) access is a reasonable alternative if IV access is not feasible or delayed.
Arrhythmias can be both the cause of and a manifestation of clinical instability. Evaluating the proximal cause of that instability will direct professionals to the most judicious use of these guidelines.
|
|---|
 |
■Significant Changes Vector Change & Double Sequential Defibrillation
|
|---|
■Evidence to Recommendation - Vector Change and DSD
 |
 |
■Significant Changes Initial Vascular Access
|
|---|
■Evidence to Recommendation – IV vs IO Access
 |
 |
■Significant Changes Vasopressor Medications
|
|---|
|
■Significant Changes Adjuncts to CPR
|
■Evidence to Recommendation – Heads Up CPR
 |
|
■Significant Changes Termination of Resuscitation Measures
 |
 |
■Significant Changes Wide-Complex Tachycardia
|
|---|
■Significant Changes
Initial Management of Bradycardia
 |
|
■Significant Changes Atrial Fibrillation of Flutter with Rapid Ventricular Response
|
■Adult Cardiac Arrest(VF/pVT/Asystole/PEA)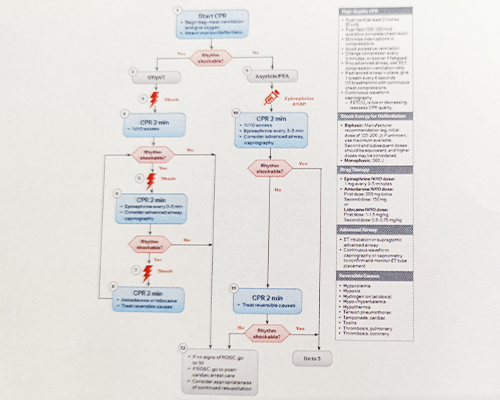 |
■Adult Cardiac Arrest Circular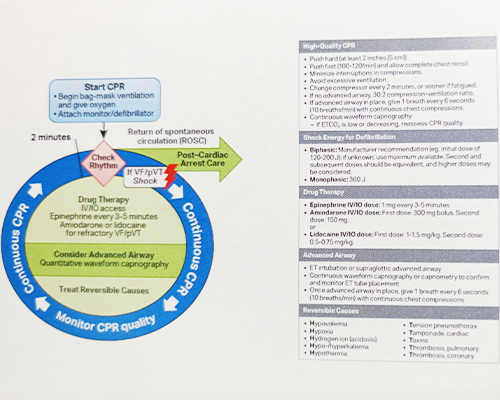 |
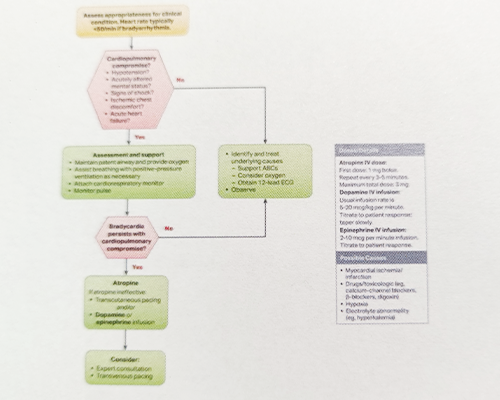
■Adult Bradycardia with a Pulse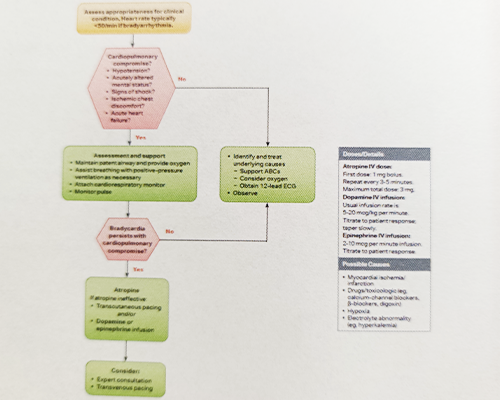 |
■Adult Tachyarrhythmia with a Pulse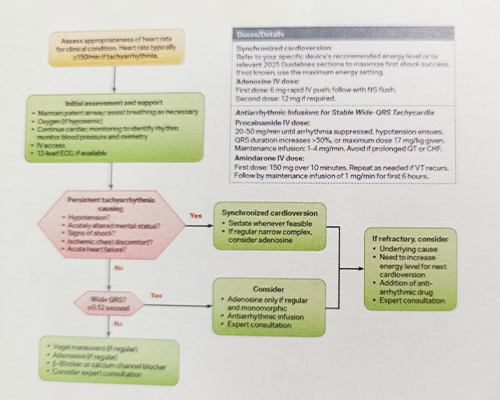 |
■Termination of Resuscitation Algorithms |
■Electrical Cardioversion Algorithm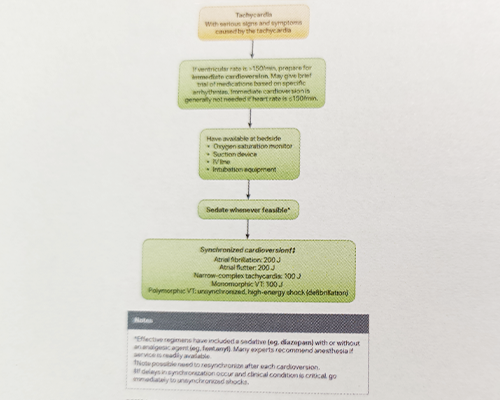 |
 |
Thank You! |
|---|
|
Pediatric Advanced Life Support (PALS) Updates |
|---|
|
■Disclosures Volunteer: American Heart Association, American Academy of Pediatrics
|
Universal Chain of Survival  |
   |
■PALS Top 10



|
|---|
|
■Significant Changes Drug Administration During Cardiac Arrest
 |
|
■Significant Changes Measuring Physiology During CPR
|
|
■Significant Changes Measuring Physiology During CPR
 |
|
■Significant Changes Post-Cardiac Arrest Management

 |
|
■Significant Changes Prognostication Following Cardiac Arrest It is recommended that health care professionals consider multiple modalities when predicting neurological outcomes (favorable or unfavorable after resuscitation from cardiac arrest in infants and children). Avoid single tests conducted in isolation and use multiple modalities at various timepoints throughout the post-cardiac arrest period for prognostication. New recommendations for prognostication:
|
■Neuroprognostication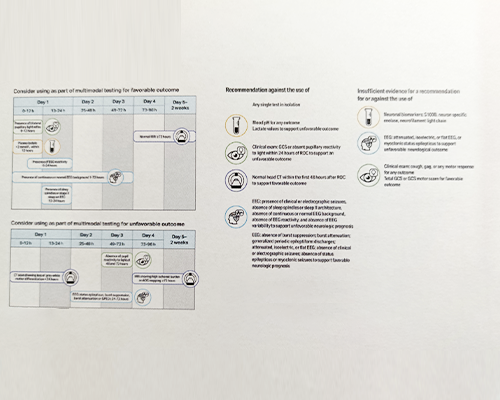 |
|
■Significant Changes Post-Cardiac Arrest Survivorship
|
|
■Updated Algorithms Cardiac Arrest 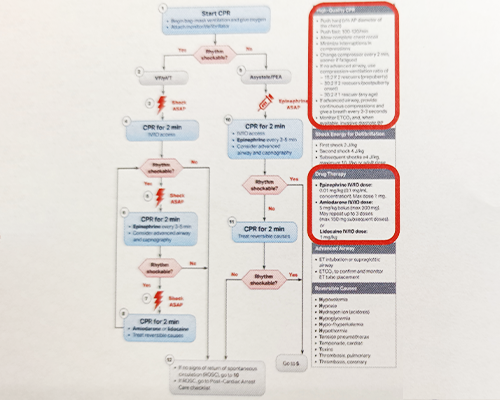 |
|
■Updated Algorithms Tachyarrhythmia With A Pulse  |
|
■Updated Algorithms Bradycardia With A Pulse 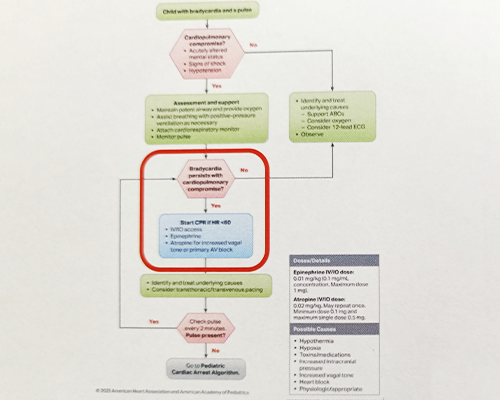 |
|
■Updated Checklist Post-Cardiac Arrest Care Checklist  |
 |
Thank You! |
|---|
|
Sience Overview Basic Life Support ■Development of the Guidelines  Class (Strength) of Recommendation
Level (Quality) of Evidence LEVEL A
LEVEL C-LD (Limited Data) LEVEL C-EO (Expert Opinion) 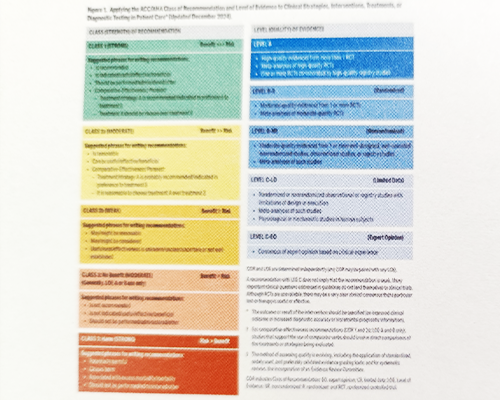 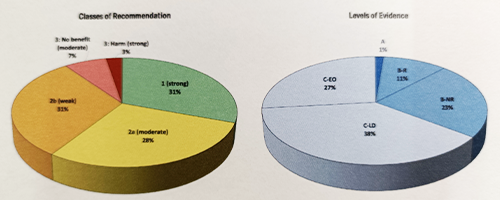 |
|---|
 |
Systems Of Care |
|---|
|
■Significant Changes Chain of Survival MAJOR CHANGE – The 4 Chains of Survival have been consolidated into one Universal Chain of Survival to include adult and peds, and IHCA/OHCA.  |
 |
Pediatric Basic Life Support |
|---|
   |
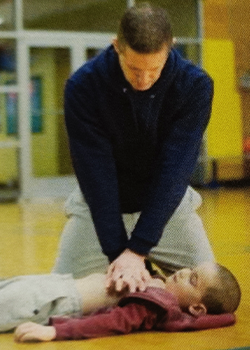
■PBLS Top 10 Immediate recognition of cardiac arrest is vital to improving outcomes. For infants and children who are unresponsive with abnormal breathing including gasping, rescuers should activate emergency medical services (EMS) and initiate high-quality cardiopulmonary resuscitation (CPR) beginning with chest compressions. High-quality CPR is the foundation of resuscitation. The key components of high-quality CPR include providing adequate chest compression rate and depth, minimizing interruptions in CPR, allowing full chest recoil between compressions, and avoiding excessive ventilation. For out-of-hospital cardiac arrest in infants and children, providing breaths in addition to chest compressions improves survival; thus, lay rescuers are encouraged to provide breaths if able and willing. A respiratory rate of 20 to 30 breaths/minute is recommended for infants and children who are (a) receiving CPR with an advanced airway in place or (b) receiving breaths and have a pulse. For infants, the recommended compression techniques include using either 1-hand technique or the 2-thumbs-encircling-hands technique. If the rescuer cannot physically encircle the chest, it is recommended to compress the chest with the heel of 1-hand technique. The use of 2 fingers along the sternum was eliminated due to ineffectiveness in achieving proper depth. For out-of-hospital cardiac arrest in infants and children, providing breaths in addition to chest compressions improves survival. For infants and children in cardiac arrest, an automated external defibrillator (AED) should be attached as soon as possible using a pediatric attenuator and pediatric pads if available. Prompt defibrillation for ventricular fibrillation and pulseless ventricular tachycardia (VF/pVT) is critical, with minimization of peri-shock pauses. For infants with severe body airway obstruction (FBAO), repeated cycles of 5 back blows alternating with 5 chest thrusts is recommended. Abdominal thrusts are not recommended in infants. In children with severe FBAO, guidance is the same as for infants, with repeated cycles of 5 back blows alternating with 5 abdominal thrusts, as opposed to solely abdominal thrusts. 

 |
|---|
|
■Significant Changes New Child FBAO Algorithm 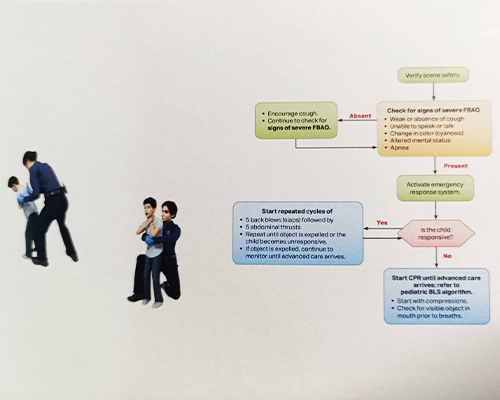 |
|
■Significant Changes New Infant FBAO 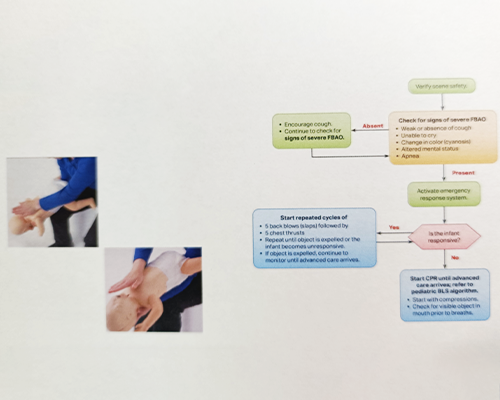 |
|
■Significant Changes Infant Choking Video  |
|
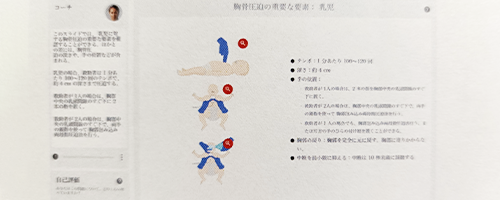
■Significant Changes Compression Technique For infants, the recommended compression techniques include using either 1-hand technique or the 2 thumb—encircling hands technique. If the rescuer cannot physically encircle the chest, it is recommended to compress the chest with the heel of 1-hand technique. The use of 2 fingers along the sternum no longer recommended due to ineffectiveness in achieving proper depth.  |
|
■Significant Changes Infant Compressions  |
|
■Significant Changes Pediatric BLS Algorithm (Infants to Puberty) for Healthcare Professionals – Single Rescuer 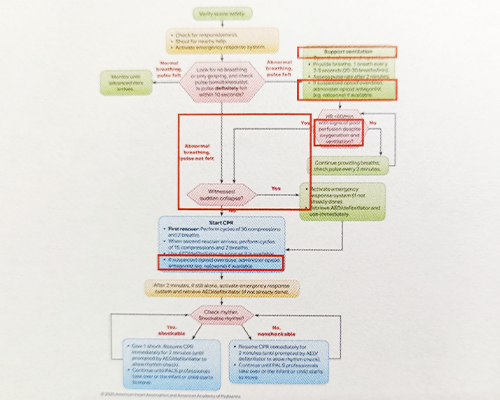 |
|
■Significant Changes Pediatric BLS Algorithm (Infants to Puberty) for Healthcare Professionals – 2 or More Rescuers  |
 |
Adult Basic Life Support |
|---|
  |
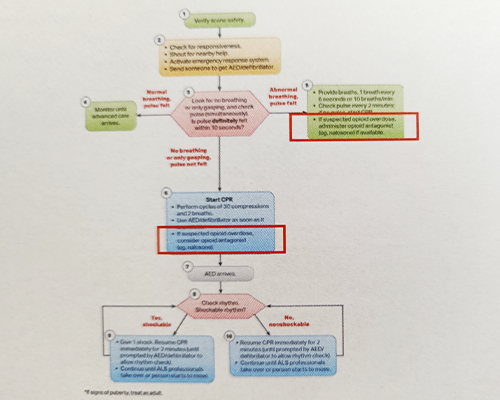
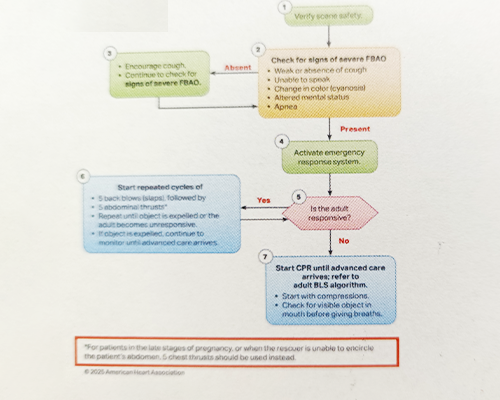
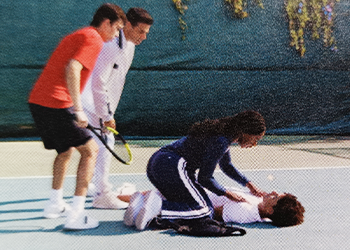
■PBLS Top 10 In adult cardiac arrest, resuscitation should generally be conducted where the patient is found, as long as high-quality cardiopulmonary resuscitation (CPR) can be administered safely and effectively. After identifying an adult in cardiac arrest, a lone responder should activate the emergency response system first, then immediately begin CPR. In adult cardiac arrest, rescuers should perform chest compressions with the patient's torso at approximately the level of the rescuer's knees. It is reasonable for health care professionals to perform chest compressions and ventilations for all adult patients in cardiac arrest from either a cardiac or noncardiac cause. When ventilating adult patients in cardiac arrest, it is reasonable to give enough tidal volume to produce visible chest rise while avoiding hypo- and hyperventilation. The routine use of mechanical CPR devices is not recommended for adults in cardiac arrest. For adult patients who are not breathing normally but have a pulse, it is reasonable for rescuers to provide 1 breath every 6 seconds (10 breaths per minute). CPR for adult cardiac arrest patients with obesity should be provided by using the same techniques as for the average weight patient. For adults with severe foreign-body airway obstruction (FBAO), rescuers should perform cycles of 5 back blows followed by 5 abdominal thrusts until the object is expelled or the patient becomes unresponsive. During adult cardiac arrest, it is reasonable for rescuers to use personal protective equipment (PPE) while performing CPR. 

|
|---|
|
■Anterolateral Pad Placement Standardized Visuals and Verbiage for 2025 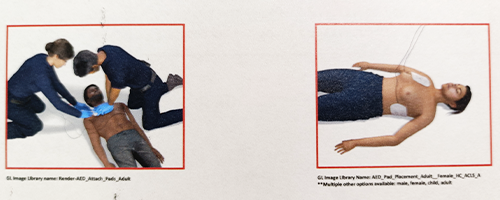 |
|
■Adult BLS Algorithm Adult BLS Algorithm for Healthcare Professionals Major Changes:
 |
|
■Adult Foreign Body Airway Obstruction New Recommendations:
 |
 |
Thank You! |
|---|
|
Training Implementation ■International: Precourse Self-Assessment (PSA) and Video Prework ACLS AND PALS ONLY
 |
|---|
■International Instructor Updates and Product & Course Orientations (P&CO)
 |
|
■Interim materials Interim materials are available on Atlas Course Information page.  |
|
■Atlas Platform Updates INTERNATIONAL USERS 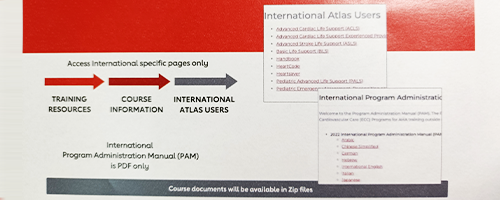 |
|
■International Exams FIND ON SHOPCPR:
 |
|
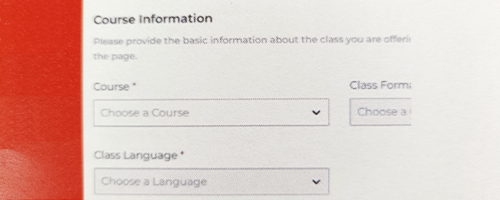
■Creating Classes on Atlas COURSE NAMES ALIGN WITH AGENDAS
 |
|
■Updated Universal Chain of Survival The 2025 Systems of Care Guidelines has a new Chain of Survival, which is intended to apply to all forms of cardiac arrest regardless of age (pediatric versus adult) or location (out-of-hospital or in-hospital). |
 |
 |
■Significant Change For infants, the recommended compression techniques include using either 1-hand technique or the 2 thumb-encircling hands technique. If the rescuer cannot physically encircle the chest, it is recommended to compress the chest with the heel of 1-hand technique. The use of 2 fingers along the sternum was eliminated due to ineffectiveness in achieving proper depth. This is a major change from 2020 where the use of 2 fingers was still a recommended technique. The removal of this recommendation also removes differences in compression technique between single and two-rescuer CPR in infants. Previously it was recommended that a single rescuer use the 2 finger technique and two-rescuers use the two-thumb technique. Now for single or two-rescuer, either two-thumbs or the heel of one hand is recommended, whichever can achieve the best depth. |
|---|
 |
■Foreign Body Airway Obstruction
|
|---|
 |
■Science Updates EXPANDED FIRST AID GUIDANCE
|
|---|
|
■Streamlined Course Paths Core Offerings
Updates
|
|
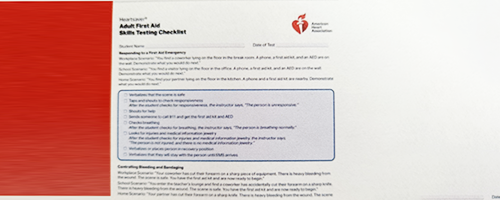
■Practice & Skills Testing Required First Aid Skills
 |
 |
■Combined Instructor Manual 2-in-1 Resource
|
|---|
|
■Combined Student Workbook 4-in-1 Comprehensive Resource
|
|---|
■Heartsaver Instructor Resources |
 |
■eLearning Dynamic and engaging
|
|---|
 |
BLS |
|---|
|
■BLS Update COURSE TRACKS BLS Provider Course is designed for health care professionals and trained first responders who provide care to patients in a wide variety of settings, as well as individuals enrolled in a health care training program. There are still 2 main course tracks for the BLS audience: in-hospital and out-of-hospital. Both tracks include the same course content, but the scenarios presented are tailored to the audience taking the BLS course. 
|
|
■Basic Life Support SKILLS TESTING CHECKLIST Infant CPR Skills Testing Checklist

|
 |
■Basic Life Support STUDENT PRACTICE ACTIVITIES Instructor-led student activities within lesson plans
|
|---|
 |
■Basic Life Support LESSON PLAN Discontinued Lesson Plans The continuous compressions lesson plan has been discontinued in the BLS course. |
|---|
 |
■Basic Life Support Update Interim materials available on Atlas Course Information page. International HeartCode Standardization for BLS provider course, Instructor training will not change. |
|---|
 |
ACLS |
|---|
 |
■Revised Course Agenda Titles ACLS agenda titles have been revised to align with the learner's chosen path—either completing the precourse self-assessment and video prework or just the precourse self-assessment alone. Agendas:
|
|---|
|
■High-Quality BLS Learning and Testing Stations Revised Continuous compressions reduced to 1 minute per student—Record how many compression performed in the 1 minute. This will reduce fatigue during the course. 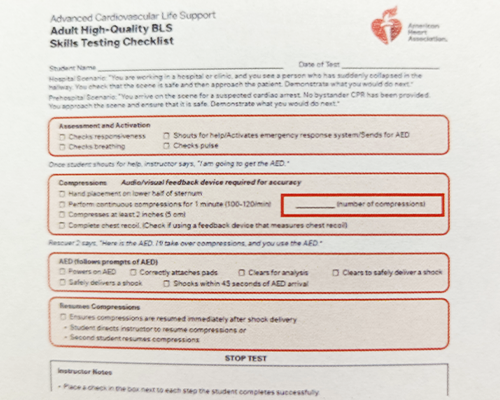
|
|
■Airway Management Skills Testing Checklist Record the exact number of average interval between breathes 
|
 |
■Megacode Testing
|
|---|
■Updated Skills Testing Checklist
|
|
■Roster Changes New column for CCF % Instructors will record the passing CCF (Chest Compression Fraction) for each student. 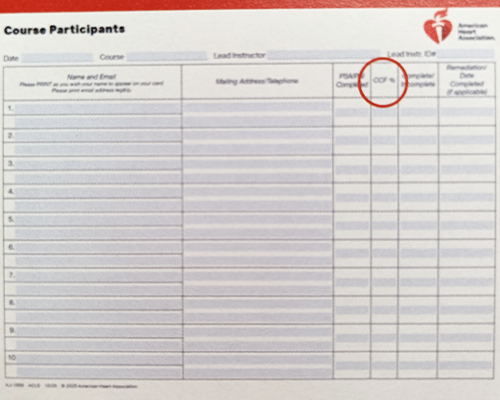
|
 |
PALS |
|---|
 |
■Lesson Plans Revised to single set of plans chosen based on agenda
|
|---|
 |
■Updated Skills Testing Checklist Updated skills descriptor regarding hand placement |
|---|
 |
■New 3 Minute Teams Dynamics Skill
|
|---|
|
Thank You! |
|---|
|
2026 AHA Guidelines Launch THE PROGRAM ADMINISTRATIVE MANUAL Marida Straccia American Heart Association International Program Administrator Manager |
|---|
|
■THE PAM CONTENTS
|
International Training Network Structure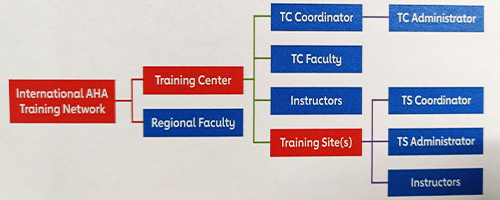
|
|
■International Training Center Organization ■THE PAM: ITC ORGANIZATION The Role of the ITC

|
■INTERNATIONAL TRAINING CENTER
|
|
■International Regional Faculty Criteria

|
|
■ITC Staffing Roles ITC Coordinator
AHA Training Center Faculty (TCF) Role
Renewal Criteria
|
|
ICT Policies and Procedures ■Managing an ITC Agreement The agreement will remain active until it expires and is not renewed or either party chooses to terminate the agreement under the terms of the ITC agreement. To ensure that each ITC meets its contractual obligations, the AHA Regional Office will conduct periodic reviews. All ITCs should adhere to the terms of the agreement and AHA guidelines outlined in this PAM. The TCC should retain a copy of the current ITC Agreement on file at the ITC. 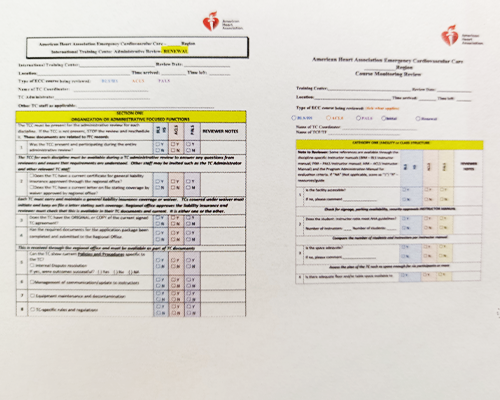
|
|
■Managing an ITC Agreement Adding a Discipline ITCs that wish to add or reinstate a discipline need to contact the Regional Director who will provide the application to submit with the appropriate documentation. Deleting a Discipline The procedure for deleting a discipline is the same as for terminating an ITC Agreement. All instructors must be notified in writing by the TCC. Liability Insurance for ITCs 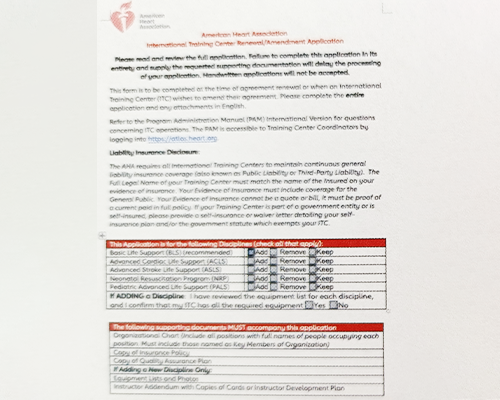
|
|
ITC Acquisitions Any change of control of an ITC, including mergers, acquisitions, or ownership transfer, requires the submission of a new ITC Application, including updated insurance reflecting the new organization. The AHA will review the new organization to ensure compliance with all applicable criteria and policies. If approved, the new organization must execute a new ITC Agreement before conducting any AHA courses. Until the new agreement is fully executed, the existing ITC Agreement cannot be assigned, transferred, or continued under new ownership. |
 |
Managing Records Document Retention ITCs must keep all required documents (either hard copy or electronic) for at least 3 years after the date of action; for example, maintain records for 3 years past the last day of the course.
ITCs that are on Atlas are not required to submit training reports. Those countries not on Atlas must submit a midyear report and an end-of-year report. Failure to submit the required ITC Activity Report by the deadline is considered a breach of the ITC Agreement and cause for the AHA to terminate the ITC Agreement. |
|---|
|
Course Fees
The AHA does not set or receive fees for courses offered by ITCs or instructors. It is the responsibility of the ITC and/or instructor to determine what fees, if any, to charge for their courses and to ensure that their billing practices comply with applicable laws. The following disclaimer must be printed on all ITC promotional brochures, announcements, agendas, or other materials distributed to students in courses for which fees are charged: The American Heart Association (AHA) strongly promotes knowledge and proficiency in all AHA courses and has developed instructional materials for this purpose. Use of these materials in an educational course does not represent course sponsorship by the AHA. Any fees for an AHA course are set and charged solely by the applicable Training Center or Training Site and are not charged by the AHA. |
|
■AHA Platforms All ITCs should fully use the AHA Platforms for maintaining course records, managing instructors, and accessing course information and exams. Users have the following access, depending on their role:
|
|
Instructor Alignment ■Requirements for Instructor Alignment An instructor candidate must complete all course and monitoring requirements and be accepted by and align with an approved primary AHA ITC that is authorized by the AHA to teach in that geographic territory before teaching a course other than the initial monitored course. Only instructors aligned with an ITC are authorized to teach courses and issue course completion cards through the TCC. 
|
|
■Instructor Status Revocation Revocation of instructor status means the privilege of claiming instructor status, aligning with an ITC, and issuing AHA course completion cards is no longer allowed. Reasons for Instructor Revocation The following list includes some, but not all, instructor activities that could result in revocation:

|
|
Boundaries and Recognition of Status ■Training Boundaries ITC Agreement The ITCs (including all aligned instructors and TSs) may offer their AHA courses only in the geographic territory defined in their ITC Agreement. 
|
|
■Training Boundaries Training Outside of the ITC’s Authorized Territory The AHA acknowledges that many AHA instructors and ITCs have ongoing relationships within the international medical and safety communities. However, an ITC’s approval to deliver AHA training is strictly limited to the Territory defined in its ITC Agreement. Any training outside that Territory requires prior written approval from AHA through the process of obtaining permission to ensure the quality of international training. 
|
|
■Recognition of Status The AHA ECC Programs recognizes the mobility of its providers and instructors and encourages them to remain active in the ECC Training Network wherever they move. International TCs The role of the ITC and US Training Center is the same. The AHA seeks consistency in training in all ITCs, both in the United States and globally. AHA course completion cards issued by any AHA ITC should be considered equivalent, regardless of their country of origin. 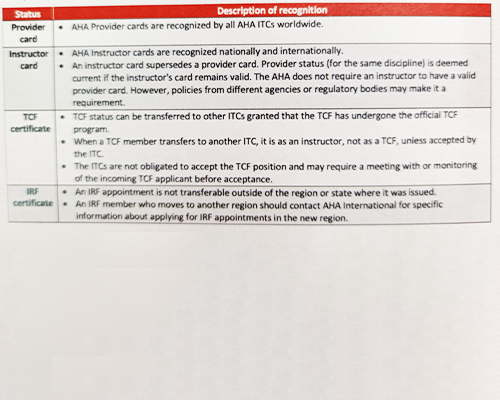
|
 |
Course Information ■Course Information General Information For specific course information, please refer to the appropriate instructor manual.
|
|---|
 |
■Use of the Term Health Care Professional in Advanced Courses The AHA uses the terminology of "any current, active health care professional" to be inclusive of any potential member of a resuscitation team. Examples of "any current, active health care professional" include but are not limited to:
|
|---|
 |
■Instructor Candidates The AHA requires that instructors be at least 18 years of age for Heartsaver Instructor Essentials. BLS, ACLS, PALS, and PEARS Instructors must be at least 18 years of age and be licensed or credentialed in a health care occupation in which the skills are within the provider's scope of practice. ITCs should ensure that they comply with local laws regarding the age of instructors and participants. |
|---|
|
Conflict of Interest and Ethics Policy ■Conflict of Interest The AHA has established a Conflict of Interest Policy that applies to all ECC leadership roles, including but not limited to International Regional Faculty (IRF), Training Center Coordinators (TCC), Training Center Faculty (TCF), and any other individuals designated by AHA as ECC leaders (ECC Leaders). Conflict of Interest Policy ECC Leaders shall avoid any conflict between their own respective personal, professional, or business interests and the interests of the AHA in any and all actions taken by them on behalf of the AHA in their respective capacities. ECC Leaders are expected to conduct themselves with impartiality while performing AHA ECC tasks. Ethics and Code of Conduct The AHA has established an Ethics Policy that applies to all AHA leaders, ITCs, and instructors. These positions hold a responsibility to exhibit a high standard of conduct. 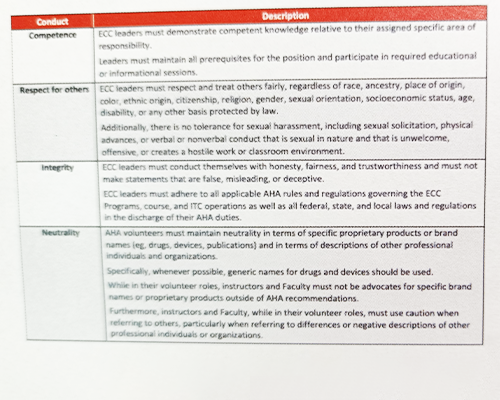
|
|
Legal Aspects ■Trademarks The AHA's stylized name and heart-and-torch logo are trademarks of the American Heart Association, Inc. and are registered with the US Patent and Trademark Office. Only the AHA may use these trademarks. The AHA has an ITC seal logo (ITC Seal) that includes the heart-and-torch logo. ITCs may use this ITC Seal logo if their use of the ITC Seal meets the requirements outlined in the Authorized ITC Seal – Guidelines for Use for TCCs. This document and the ITC Seal logo application may be requested from the AHA Regional Office and ITCAgreementSupport@heart.org. 
|
|
■Using AHA Verbiage, Logos, and Marks Instructors are not AHA employees; they operate under independent Training Centers that the Association licenses. Listing "American Heart Association" or "AHA" as an employer or in their job title on business cards erroneously implies a formal employment relationship. Inaccurate representation of their role may lead students, clients, and regulatory bodies to believe the Association is directly responsible for training quality, logistics, or business practices of these individuals and exposes the Association to liability for their actions. Instructors can use the following language on their CVs or business cards because it does not incorrectly assert or imply an employment relationship with the AHA: "Instructor authorized to teach American Heart Association courses" "Certified by an American Heart Association-licensed Training Center to teach Association courses" "Certified to deliver American Heart Association curriculum through [Name of Licensed ITC]" |
|
References and Resources ■Resources on the ECC Training Network 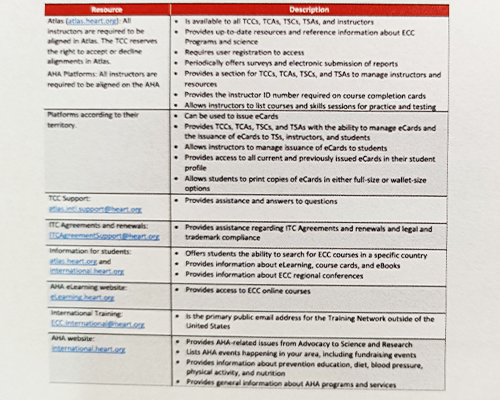
|
|
Thank You! |
|---|
 |
2025 Heartcode Basic Life Support (BLS) Marida Straccia American Heart Association International Program Administrator Manager |
|---|
|
■Course Updates Updates to the BLS Course Materials: Videos and Graphics
|
|
■Course Updates Updates to the BLS Course materials: Instructor Manual
|
|
■Overview of HC BLS Course Course Types:
|
|
■HeartCode Blended Learning The HeartCode Blended Learning program combines self-directed eLearning with Instructor-led hands-on practice and testing to provide consistency in resuscitation training and meets diverse learning needs. 
|
■HeartCode BLS
|
■True Adaptive Learning in HeartCode
|
 |
■HeartCode BLS Course Topics
|
|---|
 |
■Preparing to Take 2025 Heartcode BLS Choose your preferred language |
|---|
■Find your Provider Manual
|
■Completing the Online Session  |
■Now What?
|
|
■Success The hand-on session it's mandatory for the student to receive a Provider eCard. 
|
|
Teaching a BLS HeartCode Course ■Preparing to Teach HeartCode 
|
|
■Instructor Materials For the HeartCode hands-on session, use the Instructor materials. 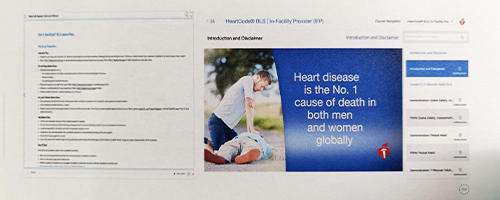 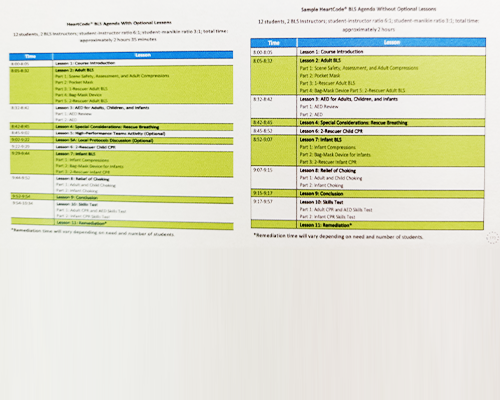  |
 |
■Hands-on Session and Skills Testing Students must demonstrate that they can successfully perform each skill as outlined in the skills testing checklists. The skills practice and testing must be conducted by an AHA Instructor for that discipline. For this session refer to the specific Lesson Plan. |
|---|
|
Instructor Development and Renewal ■Instructor Development The 5 core competencies for all instructor candidates:
|
■Instructor Essentials Course Prerequisites
|
|
■Instructor Renewal Meet the following requirements: ✓ Be renewed by a TCF ✓ Maintain current provider status ✓ Earn 4 credits during each 2 years of instructor recognition by doing any combination of the following:
|
|
Thank You! |
|---|